Endocrine System Disorders
We are discussing here only common topics from endocrine system in day to day practice.
The homoeostasis of thyroid hormone occurs through hypothalamus – pituitary – thyroid axis. The secretion of thyroid hormones (T3& T4) is controlled by hypothalamus through release of thyrotropin releasing hormone (TRH) & anterior pituitary through thyroid stimulating hormone (TSH). TSH binds to the TSH receptors on the thyroid follicular epithelium and accentuates transport of iodides from blood into thyroid follicle. The ultimate product of the process is thyroxine (T4) & triiodothyronine (T3). It is stored in the thyroid gland. When level of thyroid hormones is elevated in the blood, it stimulates negative feedback mechanism to suppress the secretion of both TRH &TSH to maintain thyroid hormone secretion.
Thyroid disorders commonly present in the form of hypothyroid, hyperthyroid & enlargement of thyroid i.e. Goiter.
Hypothyroidism is caused by either structural or functional derangement that interferes with the production of adequate levels of thyroid hormone. It results from defects anywhere in hypothalamic – pituitary – thyroid axis. Hypothyroidism is fairly common in practice affects predominantly female population.
It can be congenital, acquired or autoimmune.
Congenital hypothyroidism is the result of endemic iodine deficiency in the diet. In India it is commonly seen in northern states such as Himachal Pradesh
Autoimmune hypothyroidism is most common cause of hypothyroidism in iodine sufficient areas of the world. E.g. Hashimoto’s thyroiditis.
In some cases, hypothyroidism occur secondary to surgical or radiation induced excision of thyroid parenchyma.
The clinical presentation in early stage is usually weight gain, fatigue, menorrhagia, constipation with vague myalgia etc. Prolonged hypothyroidism produces low pitched voice, stunned speech & carpel tunnel syndrome etc. If hypothyroidism develops in infancy or early childhood, it is termed as cretinism. The child manifests with mental retardation, short stature, a protruding tongue, coarse facial features & umbilical hernia. It is important to diagnose cretinism child as early as possible because it is treatable.
Hashimoto’s thyroiditis – It is caused by breakdown in self-tolerance to thyroid auto-antigens which is represented by presence of circulating auto- antibodies against thyroglobulin & thyroid peroxidase in majority of cases.
Usually Hashimoto’s thyroiditis presents with painless enlargement of thyroid which is diffuse & symmetric associated with some degree of hypothyroidism.
In hypothyroidism free T3& T4 level decreases whereas TSH level increases to the considerable level. TPO or thyroglobulin antibodies are detectable in cases of autoimmune thyroiditis.
Thyrotoxicosis – It is a hypermetabolic state caused by elevated circulatory levels of free T3& T4. It is most commonly caused by hyperfunction of thyroid gland; it is often referred as hyperthyroidism. Thyrotoxicosis & hyperthyroidism are the terms which are used interchangeably.
Patient presents with varied manifestation of hypermetabolic state like weight loss despite of increased appetite. Cardiac manifestation like tachycardia, palpitations & cardiomegaly occur. When patient gets tremors, anxiety & insomnia, one can suspect hyperthyroidism. Ocular changes like wide, staring glance and lid lag may occur later on.
Common causes of Thyrotoxicosis –
- Grave’s disease – It is an autoimmune disease. The level of thyroid hormone increases with or without diffuse goiter. It also causes ophthalmopathy.
- Transient thyroiditis – i. Subacute thyroiditis – It is a transient inflammation of thyroid gland occurring after viral infection. It is a painful condition. The thyroid inflammation & hyperthyroidism are transient and usually diminish after 2 to 6 weeks. After recovery thyroid functions returns to normal within 6 to 8 weeks.
In few cases thyrotoxicosis occurs within 12 months after pregnancy. It is called as post-partum thyroiditis.
A diagnosis of hyperthyroidism depends upon clinical as well as lab findings. In most of the patients free T3& T4 levels are elevated with undetectable (low) level of TSH. TSH receptors antibodies (TRAb) are elevated in cases of Grave’s disease.
Goiter – It is an enlargement of thyroid gland and is common manifestation of thyroid disease with affinity for females.
Impairment of thyroid hormone synthesis leads to a compensatory rise in serum TSH level, which in turn causes hypertrophy of thyroid follicular cells and ultimately leads to enlargement of thyroid gland.
It is of 2 types –
- Diffuse nontoxic goiter causes enlargement of entire gland without nodularity. It is also called as simple goiter. It is more common in iodine deficient areas. Most of the time thyroid function is adequate but occasionally it produces symptoms because of mass effect such as dysphagia.
- Multinodular Goiter – Irregular enlargement of thyroid gland is termed as multinodular goiter. Most of the cases of long-standing simple goiter convert into multinodular goiter. The clinical features are produced because of mass effect.
Both the type of goiters are almost invariably benign in nature whereas1:20 chance of malignancy is there in truly solitary lesion.
USG of neck and radio-isotope scanning is necessary for the diagnosis.
Diabetes Mellitus (DM) – It is not a single clinical entity but rather refers to a group of common metabolic disorders characterized by hyperglycemia.
Basically, there are 2 types –
- Type I D.M. – It is the result of nearly complete insulin deficiency therefore previously termed as insulin dependent diabetes mellitus (IDDM). It is not very common in general practice.
- Type II D.M. –It is characterized by variable degree of insulin resistance, insulin secretion and increased hepatic glucose production. It is very common in clinical practice. The incidences of DM are rising in India.
Diabetes Mellitus results from a complex interaction of genetic and environmental factors.
Genetic susceptibility along with predisposing factors like obesity, lifestyle and less exercise develop insulin resistance. Insulin deficiency because of beta cell failure and excess hepatic glucose production ultimately leads to hyperglycemia.
Pathophysiology of D.M.
- Diabetes Mellitus is preceded by a phase of abnormal glucose homoeostasis. In the beginning insulin resistance develops (though exact mechanism is not known) but glucose tolerance is normal because beta cells are able to meet insulin need. At certain point beta cell are unable to tolerate excess glucose and one can find increase in post prandial sugar. After that reduction in insulin secretion together with hepatic glucose production lead to fasting hyperglycemia. At last beta cell failure occurs. All these factors together contribute to the uncontrolled blood glucose level in diabetic patient.
DM type II is more common in middle aged and elderly. It presents with variety of symptoms. The common symptoms are polyuria, polydipsia, weight loss, fatigue, weakness, pruritus vulvae, balanitis, blurred vision, frequent infection, slow healing of skin lesion etc.
Physical Examination –
- Peripheral pulses – may be abnormal
- Foot examination –look for localized infections, presence foot ulcer and fungal infection between toes.
- Ankle Reflexes – loss of reflex occurs in typical sensory motor neuropathy
- Vibratory sensation (to detect neuropathy)
- Eye examination- to check visual acuity, cataract or lens opacity. Fundoscopy is also advisable.
- B.P. measurement is also essential.
Classification
Type I Diabetes Mellitus – Onset is prior to 30-year, patient has usually lean body. There is propensity for ketoacidosis with increased risk of autoimmune disorders such as thyroid disease, adrenal insufficiency and vitiligo etc.
Type II Diabetes Mellitus – Onset is after 30 years. Patient is usually obese (80%). Patient has associated conditions such as hypertension, dyslipidemia, Cerebrovascular disease and PCOS etc.
Diagnosis
- Random blood sugar 200 mg or more Or Fasting plasma glucose is 126 mg or more
- Glycated hemoglobin is 6.5 or 2 hr. plasma glucose 200 mg after glucose tolerance test
Glycated Hemoglobin or fasting plasma glucose is most reliable for identifying D.M. in asymptomatic individuals.
Monitoring of D.M. patient is done by measuring –
- Blood sugar level – fasting and PP
- Glycated Hemoglobin – provides an accurate measure of glycemic control over a period of weeks to months.
- Lipid profile and serum creatinine (annually)
- B.P. measurement (quarterly)
- Eye examination (annually)
- Foot examination SOS
Patient commonly develops complication decade after a disease starts.
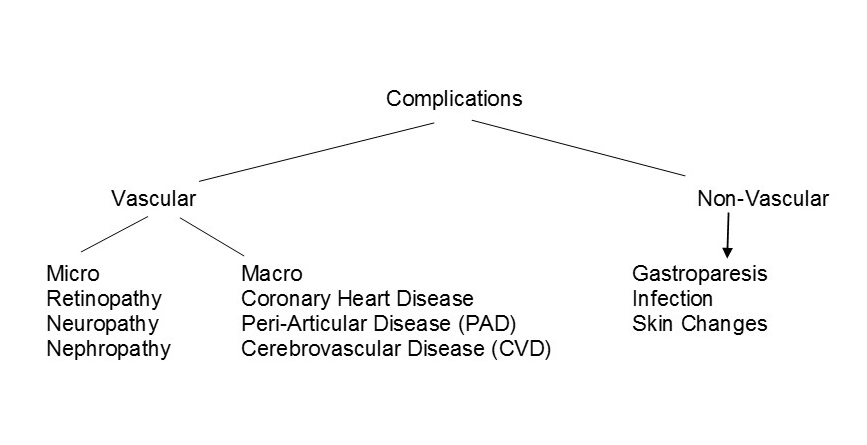
A. Ophthalmic complications –
a. Progressive Diabetic Retinopathy
It is of 2 types
- Proliferative – In response to retinal hypoxemia neovascularization develops causes vitreous hemorrhage and finally retinal detachment.
- Non proliferative – It is marked by retinal vascular microaneurysm and slowly progresses to retinal ischemia.
b. Significant macular oedema is observed in cases of non-proliferative retinopathy.
B. Renal Complication
After 5 yrs. of disease 40% of individual with DM type II develop micro albuminuria 30 – 299 / mg / dl in 24 hrs. They have a risk for cerebrovascular disease.
C. Neuropathy in D.M.
Long standing D.M. patients develop symptoms of polyneuropathy, (such as hyperesthesia, numbness, tingling etc.). Autonomic neuropathy (such as hyperhidrosis of upper extremities and anhidrosis of lower extremities) and less commonly symptoms of mononeuropathy.
D. Gastrointestinal and genitourinary dysfunction – like constipation, anorexia, erectile dysfunction, loss of libido and recurrent UTI.
E.Cardiovascular system
It is better to advice stress test if one can find symptoms of cardiac ischemia and other risk factors like dyslipidemia and HTN in diabetes mellitus patient.
F. Peripheral artery disease, neuropathy and poor wound healing are the complications of lower extremities.
G. Skin – Delayed wound healing, ulcerations and hyperpigmented spots.
H. Frequency and severity of infections increases in diabetes patients because of abnormalities in cell mediated immunity.
Management –
General Advice on Diet, Exercise and avoidance of risk factors like smoking are necessary.